Transfusion medicine
Transfusion medicine handbook
The Transfusion Medicine Handbook is designed to assist hospital staff and other health professionals in modern Transfusion Medicine Practice.
5. Fractionated Products
5.4.10 PRIVIGEN NZ / PRIVIGEN (Normal Immunoglobulin) 10% intravenous immunoglobulin (IVIg)
Privigen is a sterile, preservative free 10% solution containing 10 g of human protein in 100 mL, available in 50 mL (5 g), 100 mL (10 g) and 200 mL (20 g) vials. The solution has a pH of 4.8 and is approximately isotonic. The product contains L-proline as a stabiliser which is a physiological non-essential amino acid. It contains no carbohydrate stabiliser (e.g., sucrose, maltose) and has a low sodium content. Privigen is made by a combination of cold ethanol fractionation, octanoic acid fractionation and anion exchange chromatography of large pools of human. Privigen is intended for intravenous administration.
Privigen contains only trace amounts of IgA (typically <0.025 mg/mL). The manufacturing process contains specific steps to reduce the possibility of virus transmission including filtration and incubation at low pH.
NZBS stocks two Privigen products:
- Privigen NZ, produced from New Zealand plasma, is the product of choice for patients who require long term treatment. This includes patients with primary immunodeficiency and chronic neurological disorders such as CIDP. Vial sizes are 5g, 10g and 20g (round doses to multiples of 5 to prevent splitting of vials). This is the only product available at non-NZBS managed sites.
- Privigen, a commercial lVIg produced from paid donor plasma. This is held only at the 6 NZBS Blood Banks. It is used for patients receiving short term (3 months or less) or intermittent treatment with IVIg. This includes patients with ITP, Guillain Barré and Kawasaki disease. Privigen is the commercial alternative to Privigen NZ with the difference being the plasma source.
Indications for Use
Privigen is registered for use as replacement IgG therapy and immunomodulatory therapy for a number of conditions.
Table 5.16: Registered Indications for Use of Privigen
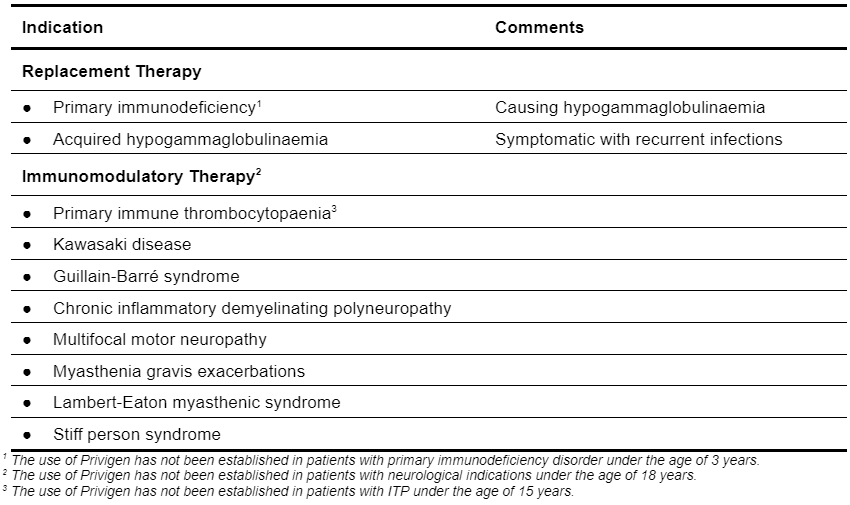
In addition, intravenous immunoglobulin (IVIg) has an established and emerging therapeutic role in a wide range of other autoimmune and inflammatory diseases. Privigen is not registered in New Zealand for indications other than those listed. For situations involving off-label indications, issue of this product is subject to consultation between the specialist physician and a NZBS Transfusion Medicine Specialist/ Medical Officer.
Comprehensive evidence-based guidelines for the use of intravenous immunoglobulin are lacking. Substitutes, such as the Criteria for the Clinical Use of Intravenous Immunoglobulin in Australia (the Criteria) https://www.criteria.blood.gov.au/ and the Clinical Guidelines for Immunoglobulin Use https://www.gov.uk/government/publications/clinical-guidelines-for-immunoglobulin-use-second-edition-update provide guidance about recognised uses.
Dosage and Administration
Privigen is supplied in a glass vial (bottle) and requires a vented infusion set to administer. The solution contains no antimicrobial preservatives; each bottle must be transfused within 4-hours of spiking (breaking the product seal with the IV set spike).
Privigen may be infused undiluted. It may also be infused diluted with 5% glucose. It cannot be diluted in saline – saline solutions destabilise the product causing it to precipitate.
- Patients naive to Privigen, switching from an alternative IVIg product, or who have not received IVIg for a long time, should be closely monitored during and for the first hour after the first infusion. The maximum rate may not be tolerated by all patients.
Rate of Administration – Titration Schedule
- All infusions should be commenced at the rate of 0.3 mL per kilogram body weight per hour(mL/kg/hour).
- If well tolerated, the rate may double every 30 minutes to a maximum of 2.4mL/kg/hour for the first three infusion episodes. If a dose is divided over more than one day, that is classified as one episode. The maximum rate may not be tolerated by all patients.
- From the fourth infusion, titrations continue to be at 30-minute intervals; the rate however can be increased beyond 2.4mL/kg/hour, with two further titrations to a maximum of 4.8mL/kg/hour.
- In patients at risk for acute renal failure or thromboembolic adverse reactions, IVIg products should be administered at the minimum rate of infusion and dose practicable.
IVIg Vital Signs
- Baseline respiration rate, heart rate, blood pressure and temperature should be recorded before commencement.
- For the first 15 minutes of the infusion closely monitor the patient, repeating the IVIg vital signs at 15minutes, then every 15 minutes thereafter for the first hour.
- Repeat the IVIg vital signs twice in the next hour, then hourly until the infusion is completed.
- Monitor the patient post infusion for evidence of an adverse reactions.
Replacement Therapy
- The optimal dose and frequency of administration of Privigen must be determined for each patient.
- Most patients receive 400 mg IgG per kilogram body weight initially, followed by monthly maintenance doses of at least 200 mg per kilogram body weight.
- The monthly maintenance dose, guided by the patient's clinical status, is often 300 - 450 mg of IgG per kilogram body weight aiming for a pre-infusion (trough) serum IgG level of at least 4 - 6 g/L.
- As catabolic rates vary, the IgG levels of new patients should be monitored regularly for several monthly cycles to determine the effective dose. Three to six months are required for equilibration.
Immunomodulatory Therapy
Primary Immune Thrombocytopenia
- Patients should receive up to a maximum total cumulative dose of 2.0 g IgG per kilogram body weight, over 2 - 5 days.
Kawasaki Disease
- Patients should receive 1.6 - 2.0 g IgG per kilogram body weight, administered in divided doses over 2 - 5 days, or 2.0 g IgG per kilogram body weight as a single dose.
Guillain-Barre Syndrome
- Patients should receive 0.4 g IgG per kilogram body weight per day for five days.
Chronic inflammatory demyelinating polyneuropathy
- Patients should receive a starting dose of 2.0 g IgG per kilogram body weight, administered in divided doses over 2 - 5 days.
- Patients should receive a maintenance dose of 1.0 g IgG per kilogram body weight, administered every three weeks.
Multifocal motor neuropathy
- Patients should receive a starting dose of 2.0 g IgG per kilogram body weight, administered in divided doses over 2 - 5 days.
- Patients should receive a maintenance dose of 0.4 - 2.0 g IgG per kilogram body weight, administered every two to six weeks.
Myasthenia gravis exacerbations
- Prior to surgery or during myasthenic crisis patients should receive an induction dose of 1.0 - 2.0 g IgG per kilogram body weight, administered in divided doses over 2 - 5 days.
- Patients should receive a maintenance dose of 0.4 - 1.0 g IgG per kilogram body weight, administered every four to six weeks.
Lambert-Eaton myasthenic syndrome
- Patients should receive a starting dose of 2.0 g IgG per kilogram body weight, administered in divided doses over 2 - 5 days.
- Patients should receive a maintenance dose of 0.4 - 1.0 g IgG per kilogram body weight, administered every two to six weeks.
Stiff person syndrome
- Patients should receive a starting dose of 2.0 g IgG per kilogram body weight, administered in divided doses over 2 - 5 days.
- Patients should receive a maintenance dose of 1.0 - 2.0 g IgG per kilogram body weight, administered every four to six weeks.
IVIg dosage recommendations for off-label indications are available in Criteria for the Clinical Use of Intravenous Immunoglobulin in Australia (the Criteria) https://www.criteria.blood.gov.au/
Contraindications
Privigen is contraindicated in individuals who have had a true anaphylactic reaction to the active substance or the excipient and in those with hyperprolinaemia.
Precautions
- Administration
Privigen should only be administered intravenously. IVIg may, on rare occasions, cause a precipitous fall in blood pressure and a clinical picture of anaphylaxis. Therefore, adrenaline and oxygen should be available for the treatment of such an acute reaction. - Aseptic meningitis
Aseptic meningitis syndrome has been reported to occur infrequently in association with IVIg treatment, but may occur more frequently with high-doses (≥2 g/kg) and/or rapid infusion. Patients with a recurrence of aseptic meningitis syndrome in association with IV Ig treatment should be monitored for the emergence or worsening of symptoms that may indicate progression to brain oedema (cerebral oedema). - IgA antibodies
Privigen contains trace amounts of IgA which may provoke anaphylaxis in patients with IgA antibodies, such as those with IgA deficiency. - Positive direct antiglobulin tests and red cell haemolysis
Positive direct antiglobulin tests and red cell haemolysis have been reported following high dose infusion of intravenous immunoglobulin due to the presence of anti-A, anti-B, and occasionally with anti-D or other erythrocyte antibodies in the product. Such red cell sensitisation may cause crossmatching difficulties and transient haemolytic anaemia. - Renal dysfunction
There have been reports of renal dysfunction and acute renal failure in patients receiving IVIg. Patients should be adequately hydrated prior to administration of IVIg. - Thromboembolism
Thrombotic events have been reported in association with IVIg therapy. Caution should be exercised in prescribing and administering Privigen in in patients with pre-existing risk factors for thrombotic events.
Adverse Reactions
Reactions to intravenous immunoglobulin tend to be related to the infusion rate and are most likely to occur during the first hour of the infusion. It is recommended that the patient's vital signs and general status be monitored regularly throughout the infusion.
The types of reactions include: malaise, abdominal pain, headache, chest-tightness, facial flushing or pallor, hot sensations, dyspnoea, non-urticarial skin rash, itching, arthralgia, tissue swelling, hypotension, nausea, or vomiting. Should any of these reactions develop during infusion of Privigen, the infusion should be temporarily stopped (5 - 10 minutes) until the patient improves clinically and then cautiously recommenced at a slower rate.
Allergic reactions are most likely to occur during the first hour of the infusion.
True hypersensitivity reactions to intravenous immunoglobulin such as urticaria, angioedema, bronchospasm or hypotension occur very rarely. Should an anaphylactic reaction to Privigen develop, the infusion should be stopped and immediate treatment instituted with adrenaline and oxygen.
Interactions with Other Medicines
Passively acquired antibody can interfere with the response to live attenuated virus vaccines such that vaccine administration should be deferred for at least 3 months. In the case of measles and varicella vaccines following IVIg products, the impairment may persist for up to 12 months. Where deferral is impractical, patients receiving such vaccines should have their antibody response checked. By the same token, immunoglobulins should not be administered for at least two weeks after live attenuated vaccines are given. Consultation with a NZBS Transfusion Medicine Specialist/Medical Officer is recommended.